A recent story hit my newsfeed – and hit it over and over again – about how “New research shows that cannabis can prevent or treat COVID!” Examples can be seen here, here, and here.
Cannabis is often touted as a ‘cure-all’, and while there is indeed a wide range of verified therapeutic properties associated with cannabis use, there is also no shortage of anecdotal claims that are, well, bullshit. As someone who wrote and defended a PhD dissertation about how cannabinoids are working inside of our bodies, these claims tend to get under my skin probably more than they rightfully should.
The headlines I read about cannabis and COVID definitely caused my well-honed bullshit-meter to tingle, but the story was being so widely reported that I decided to give it the benefit of the doubt and actually read the full study being cited by these news outlets with an open mind. For the reader’s convenience, the study in question by 5 researchers at the University of Lethbridge can be found here.
Red Flags
Before even reading the article, there were a few glaring things that stuck out to me:
- The article is published in the multidisciplinary journal PrePrints. As a scientist, I am using the term ‘journal’ pretty loosely in this case because PrePrints is not peer-reviewed. In effect this means that scientists and clinicians will not take these results very seriously, and with good reason. These are only preliminary research findings and should not be confused for a legitimate scientific study. Note that I don’t have an issue with a ‘preprint’ format per say, but I firmly believe that these types of early data should be used to drive further research, rather than to generate any conclusions from it.
- All of the Canadian-based authors, including Dr. Igor Kovalchuk, CEO and controlling shareholder of the Alberta Research and Development company (“Swysh”), have conflicts of interest, which they disclose at the end of the article, as Pathway Research and Swysh are startup companies engaged in the cannabis and cannabinoid drug development space. [See Editor’s Note at the end of this article.]
- From the abstract I see that the experiments were performed solely in artificial cell culture models. Not so much as a single human or animal has been tested to back up any of their conclusions. There is frequently a massive gap between what we observe in a plate of cultured cells vs. what happens in animal models vs. what we observe in a real human.
Then I read the paper. It’s well written enough so that it’s easy to tell it was written by a real scientist, albeit with some poorly designed experiments and perhaps misguided conclusions. At best, the study provides an interesting preliminary preclinical finding that warrants additional study. But the news headlines grossly exaggerated conclusions from some very simple preliminary data. The article as it currently stands (in my opinion) would be highly unlikely to make it past peer-review and into a respected scientific journal. Any second-year biochem grad student worth their salt should be able to tear these experimental data apart and expose many flaws.
The ACE2 Protein
Let’s break down the experiments as if we were assigned to peer review this study. Not everyone is a scientist so we should probably do a little background science lesson to get started. SARS-CoV-2 (aka COVID-19) is a virus, an unimaginably small thing that needs to find a way to get past our body’s defenses and inside of our cells in order to propagate and stay ‘alive’ (for lack of a better lay term). The virus mainly does this by boring its way into cells through a protein that is found on the surface of our cells. Known as angiotensin-converting-enzyme-2 (ACE2), this protein is most prominently expressed in lung tissue. Once inside, the virus ‘tricks’ our cells into making more copies of the virus, the process repeats, and the infection spreads.
The researchers’ claims are speculations on human implications based on how cannabis extracts affected ACE2 levels in a cell culture dish. They grew cells in a plastic plate and aggravated these cells by adding some inflammatory cytokines to induce inflammation, then treated the cells with various cannabis oil extracts and looked at the level of ACE2 RNA and ACE2 protein found in these cells.
RNA is translated into protein by our cells, so having more RNA around often means there will also be more protein, but it’s definitely not always the case. If there is less ACE2 protein being expressed, the authors speculate, then this will lead to decreased susceptibility to the disease as there will be less entry points for the virus to enter a cell.
Fudging the Figures
Going over every figure in detail is probably excessive for the purpose of this article, so let’s just pick out one figure and give it a scientific peer review. In my opinion, Figure 2 is the most egregious. Figure 2 is broken down in to three parts, (2A, 2B, 2C).
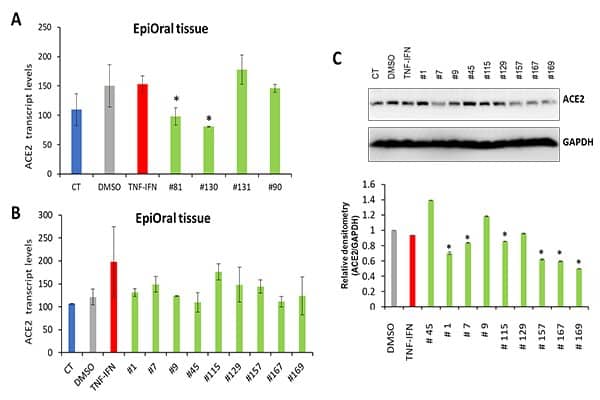
Starting with 2A and 2B, the bars on these two figures are representing the amount of ACE2 RNA being expressed in the cell culture in the various treatment conditions. Of the 13 cannabis oils tested, two of them (extracts #81 and #130) were concluded to significantly reduce the amount of ACE2 RNA found in these cells. However, I can’t seem to find any difference between the experimental conditions between 2A and 2B, so they should really be put together into a single figure and the data analyzed as a set. But notice how the control condition (DMSO) came out to be quite a bit higher in 2A than in 2B. In my view, the inconsistency of these controls undermines the credibility of the whole experiment. Further, I have a feeling that the weak statistical significance observed in 2A might be lost if the dataset were analyzed the ‘correct’ way in its entirety.
Unfortunately, we can’t know this for sure as the researchers do not actually disclose the statistical methods that were used, only stating that these datasets were analyzed using an ‘ANOVA-like’ analysis. It is critical for scientific papers to be crystal clear about the statistical models that are being utilized. An ANOVA would be appropriate in this case, but I don’t know what an ‘ANOVA-like’ analysis is – I suppose it’s almost like a real statistical method! Further, the text tells us that these experiments were repeated only twice and an n=2 is typically not deemed suitable by most journals for statistical analysis on this sort of data.
Filtered Findings
On to Figure 2C. Instead of looking at RNA, we are now looking at the actual amount of ACE2 protein that was found in these cultured cells. The researchers used a very common lab technique known as a Western Blot, which can measure the amount of protein in cells. Basically, you break open the cells, collect all the proteins, and filter them by size through a porous gel. An electrical current pulls small proteins through the gel, while larger proteins get stuck. Antibodies are then used to identify a particular protein of interest, such as ACE2.
What is shown in the first part of Figure 2C is an image of relevant portions of this gel. Darker bands generally correspond to more protein, but if you had more cells to start with then obviously you will get more protein! Researchers need a control condition if we want to compare results from different cultures. In order to account for this, we will typically include another protein in the analysis, known as a ‘loading control,’ which demonstrates equal loading of samples across all experimental conditions. Proteins such as GAPDH serve as an excellent loading control, as this protein is stably and constitutively expressed across most tissues and cell types.
The loading control shown in Figure 2C is way overloaded, as indicated by the completely black smear in the GAPDH condition, so it’s impossible to tell if there truly is reduced ACE2 protein expression or if there were simply different amounts of total protein loaded into the Western Blot. The blot data was then quantified through densitometry (Fig. 2C, bottom), which essentially compares the darkness of the band associated with your protein-of-interest vs. the darkness of the loading control in order to quantify relative abundance of protein in each respective sample.
Densitometry should NOT be performed when you have an overexposed loading control, and therefore it should not have been performed here. It was performed, though, and the researchers posit that several of their cannabis strain extracts resulted in significant downregulation of ACE2 protein. Among them is strain #1, which highlights the absurdity of their conclusions. To my eyes, extract #1 shows the second-darkest band of the sample set, meaning that there should be more ACE2 in this sample compared to the control. However, from the densitometry analysis they conclude that strain #1 resulted in significant reduction of ACE2, which is very obviously not the case through a simple qualitative assessment of their gel image.
It’s also worth noting that the extracts that caused an increase in ACE2 protein were not marked as being significantly different from the control, even though some of the samples (#45 in particular) showed such a stark increase that they almost certainly achieved statistical significance. So, their figure shows us that some strains are actually causing an increase ACE2 expression. By the authors’ own logic that means some cannabis strains will actually be harmful if taken for COVID! Of course, there’s no way to know if the cannabis you have stashed in your closet at home would increase or decrease ACE2 levels, as all of the strains tested in this paper are proprietary property developed by the authors’ company.
Haphazard Experiments
The other experiments that are outlined in the Preprints paper more-or-less repeat the experiments discussed above using different types of cultured cells. However, their choice of experiments seems haphazard, as if they’re fishing for correlations rather than methodically assessing a hypothesis. Figure 2 looked at levels of ACE2 RNA and protein to assess its level of expression in a model of oral cells, while Figure 3 looked at ACE2 RNA (but not protein) in tracheal/bronchial cells, and Figure 4 looked at ACE2 expression (back to quantifying both RNA and protein) in a model of intestinal cells.
There seems to be little logic in the strains that were chosen to test in one model to the next. Why would the strains that showed significant reduction of ACE2 in respiratory cells (#5, #10, & #31) not also be tested in any of the oral or intestinal models? Why not look at protein expression like was done for the other models? Even within the same cell type there are strange inconsistencies, such as strains #81 and #130 being the only extracts that showed significant reduction in ACE2 RNA (Fig. 2A) and they were not even included as strains tested at the protein level (Fig. 2C). It makes no sense!
Even when the same strains were tested amongst different models, I feel there should have been some discussion from the authors pointing out that they observed totally different effects between the different cell types. For example, strain extract #45 was shown to significantly decrease ACE2 in the intestinal model (Fig. 4) and drastically increase ACE2 in the oral cell culture model (Fig. 2). This seems like an important omission from the discussion. After all, lung-derived cells weren’t even tested, so how do we know that these strains don’t actually increase ACE2 expression in our lungs, the main site of entry for COVID-19? The answer is that we don’t.
I also feel the authors should have discussed that they found absolutely no correlation to the CBD or THC content in the strains that showed efficacy in their experiments. If there are indeed real effects caused by these cannabis strains, then it is almost certainly due to something in the extracts other than the major phytocannabinoids. Perhaps it’s the terpenes or flavonoids? Or perhaps we are just observing statistical chance due to improper repetition of experiments. If you tested enough different olive oil extracts, I’d venture to guess that you would also find significant effects on ACE2 expression from some of them. Effects that are ‘real’ are discerned through proper repetition and complementary experimentation, which I find lacking in this paper.
Sure, it’s feasible that cannabis reduces ACE2 expression and thereby lowers infectivity of COVID-19, but the data presented here give me very little confidence in that conclusion. Even if the experiments were performed to the point where I was completely convinced that ACE2 was truly being downregulated in human cell culture by treatment with cannabis oil, it is a HUGE freaking leap to assume that this would have any bearing whatsoever in a real-life in vivo setting.
Unvetted Science
Lastly, I’d like to note that I am not making any accusations of misconduct on behalf of the research group at Lethbridge. It is within their rights to publish the research data that they generated wherever they’d like. Though, I will mention that there are some fairly damning allegations made in the past against this group, with three of their publications being featured in PubPeer, an online forum that helps scientists to expose misconduct. But I cannot speak to those previous articles and they remain unretracted in their respective journals.
While I think there are some glaring flaws in the present article, I cannot conclude that there is any obvious misconduct or unethical behavior on the side of the researchers (aside from perhaps glossing over some points that would be inconvenient to their narrative). Though I did find it strange how frequently a hypothetical ‘cannabis mouthwash & throat gargle’ was repetitively mentioned throughout the article. If I were of a more suspicious nature, this might cause me to speculate that the authors were prepping a new product launch for their company with this PrePrints paper. It’s likely not the case, but if a Swysh/Pathway Research cannabis mouthwash hits the Canadian dispensary shelves anytime soon, then I may reconsider my take on the ethics at play here. [See editor’s note below.]
In my view it is the news outlets that are responsible for misrepresenting research in their never-ending quest for clickbait headlines. Journalists should be held responsible for vetting scientific articles prior to making clinical claims from preclinical research, particularly from this sort of very preliminary research that has not even gone through the peer-review process. A trained scientist will easily see through this for what it is, but the writing style and format used by Preprints will look like ‘official’ scientific research to the vast majority of the population, even if there’s nothing particularly noteworthy being presented.
Unvetted science is fueling COVID-19 misinformation. It is dangerous, and the problem permeates to many other societal topics today aside from COVID. It deeply frightens me that now we even have a U.S. president who routinely denounces real science and scientists in order to literally make up whatever ‘facts’ happens to suit his agenda.
More than ever, we need the critical eye of scientists during the peer-review process to help vet the bullshit. Peer-review is far from perfect, but it is the best system available for us to prevent flawed or inaccurate research from reaching readers who have not had the training to be capable of properly evaluating it.
Despite the news headlines that you may have read, this cannabis scientist will tell you that we are still a very far way off from considering cannabis as a legitimate candidate for preventative or therapeutic treatment of COVID-19 infections.
EDITORS NOTE (June 15, 2020): Project CBD has learned that the Preprints manuscript in question was submitted and posted online one month after a patent was filed on the Swysh mouthwash that is overtly peddled in the PrePrints article. This was not disclosed by the authors of the PrePrints article, a ploy that suggests the PrePrints article is more a glorified investor pitch than a legitimate scientific report. Thanks to neuroscientist Greg Gerdeman for bringing this patent application to our attention. “It really makes me question the ethics of how preprint ‘journals’ operate,” says Gerdeman.
Dr. Matt Elmes is a cannabinoid scientist and cannabis enthusiast. His professional background spans both academia and industry. He currently works as a freelance consultant for biopharmaceutical and cannabis companies. © Copyright, Project CBD. May not be reprinted without permission.
Recommended Readings

Data Distortion: Use & Abuse of Cannabis Science
Misinformation can masquerade as science, especially when it comes to cannabis. Learn how to spot faulty research.
Injecting Uncertainty into Science
Preclinical studies don’t always provide precise, controllable, and translational models for human diseases.
Cannabis Science: What to Believe
Bias is baked into scientific research about cannabis. How can you tell what is worth reading, and what isn’t?